Expert Guide to Treating Football Injuries
Treatment and Rehabilitation of Hamstring Injuries
Most of the time, specifically if the hamstring strain is first-degree, the body will respond well to R.I.C.E: Rest, Ice, Compression and Elevation. With these minor injuries the healing process is quick and there is no need for a specific programme to aid with the rehabilitation back into sport. However, players who suffer from first-degree muscle strain are advised to examine the underlying reasons for why they have become injured so as to prevent further injury. 
Regardless of the severity of the hamstring injury, the treatment is always the same. The limb should be rested in an elevated position with a padded ice pack for at least 20 minutes every 2 hours. This may not always be practical but it is an important part of the healing process which, if ignored, will extend the healing time. A compression bandage or thigh support can help with the immediate local pain. This can also reduce the swelling and when used in combination with ice packs is highly effective at minimizing pain and helping to regain normal mobility.
This form of injury also benefits from rest and if not rested the injury can become much worse. A first-degree injury, if left unattended or allowed to be used in further sports, can quickly become a second-degree strain. Similarly a second-degree can quickly become a third-degree injury.
When examining a patient who has suffered from any muscle strain it is crucial to establish a clear diagnosis of the type of injury suffered. Reviewing medical notes is important to get an indication of past injuries, specifically previous back and thigh problems, as well as any possibly related underlying medical conditions. MRI scans should be requested andcan confirm the amount of damage to the muscle and if there is an avulsion of the tendon, (where the injured tendon has pulled away small pieces of bone).
Rehabilitation should include resistance exercises and stretching as this gently helps to align the scar tissue that forms during the healing process. This alignment of the scar tissue along the stress lines of the muscle allows the strength of the hamstring to be retained. If aligned against the muscle fibres, it will become weakened and the possibility of re-injury is increased. Resistance training has the added advantage of allowing the player to remain at a competitive level of fitness. As the rehabilitation continues and the patient continues to make progress, the repetitions of the stretches are increased and core-strengthening exercises are introduced.
The severity of the injury will dictate the length of recovery and rehabilitation time. Someone with a first-degree injury may be able to return to a lower level of activity such as jogging within 7 to 9 days and sprinting within 3 weeks. With a third-degree injury the return to this reduced level can take upwards of 3 months. It is important when returning to sport to ensure that the player is able to compete effectively and without a risk of repeated injury. If this recovery process is not adhered to, the return to sport can be delayed and in some circumstances the injured player may not be able to compete at the same level as before.
Metatarsal Fractures caused by Playing Football
Another extremely common footballing injury is fracture to the 5thmetatarsal in the foot. This kind of injury has been very prevalent over recent years with many high- profiled footballers including David Beckham, Ashley Cole, Steven Gerrard and Wayne Rooney all sustaining a metatarsal injury. Metatarsal bones are long and slender and they help in balance, in holding up the body like a rigid lever and in the propulsion of the ankle and the foot.
Metatarsal fractures can be caused by activities such as landing from a jump, a forceful impact to the outside of the foot or when rolling an ankle (ankle sprain).This condition typically gives rise to a sudden onset of sharp, intense outer foot or ankle pain at the time of injury and sometimes there will be an audible snapping sound. Individuals with a 5th metatarsal fracture may also experience swelling, bruising, stiffness and pain on firmly touching the affected region of bone. An X-ray is usually required to confirm the diagnosis and to assess the severity of the fracture and further investigations such as an MRI, CT scan or bone scan may also be required.
Unfortunately, there is little that can be done to prevent a metatarsal fracture, especially when force is applied to the foot during a traumatic injury. But in football, it is felt that the lower leg shape and the alignment of the leg and the foot exacerbate the risk of injury. This is because many footballers are slightly bow-legged and this probably creates additional stress on the outside of the foot and ankle. This is really just a simple fact of mechanics. If you imagine a bow leg, and you turn the foot inwards, there is naturally an increased stress on the outside of the foot, which in this instance means an increased stress on the 5th metatarsal.
Patients with a fractured 5th metatarsal usually make a full recovery with appropriate management (whether surgical or conservative) and a return to football usually takes place in within weeks to several months.
Rectus Femoris Injuries caused by Playing Football
Injuries to the rectus femoris muscle in the front of the thigh also occur frequently as a result of playing football.
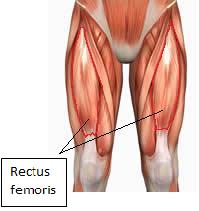
The rectus femoris muscle is one of four quadriceps muscles and is composed of fibres that are designed for rapid and forceful activity. These characteristics may explain why this muscle is particularly vulnerable to eccentric stress forces and forceful movements such as when starting to sprint or kicking a ball.
When the rectus femoris is strained, or tears, the player immediately feels pain at the top of the thigh, and in extreme cases there is a noticeable defect when the muscle is completely torn. Fortunately complete tears are rare. An MRI scan is normally requested to determine the extent of the injury.
Treatment and Rehabilitation of Rectus Femoris Injuries
Immediate application of the RICE principle (Rest, Ice, Compression and Elevation) to the thigh is required. I often use a “Myotrain” Brace from Bauerfeind, which provides cryotherapy and compression. The aim of this treatment is to reduce bleeding and damage within the muscle, which is an important part of the healing process. In addition, it helps to make the player more comfortable immediately after the injury. Depending on how much pain the player is experiencing simple pain killers like Paracetamol may be used, although try to avoid non-steroidal anti-inflammatory drugs.
Once the swelling has reduced, and sufficient movement has been restored so that the player can move around with a normal gait and range of motion the acute phase of the injury has ended. Now is a good time to exercise the quadriceps muscles, however, without inflicting additional damage or stress. This usually involves exercises where the body is supported and the weight kept off the limb, such as swimming or cycling.
From this point gentle resistance exercises and thigh stretching is important, as this helps to align the scar tissue that will have formed during the healing process. By aligning the scar tissue along the normal lines of stress the tensile strength of the thigh muscle is enhanced. Finally, core strength and stability exercises can improve muscle function across the trunk and pelvis, which can help reduce the risk of re-injury. Recovery must be closely monitored, so that improvements can be noted and the rehabilitation programme altered to aid the recovery process.
It is difficult to estimate the length of time to full recovery. Some athletes will be performing normally within 1 to 4 weeks, but occasionally it can take 6 to 8 weeks or more, this depends on the extent of the injury, the health of the individual and any underlying medical conditions.
Preventing Rectus Femoris Injuries
Warming up decreases muscle stretch injuries in players because the muscles are more extensible when the tissue temperature has been increased by a few degrees above normal. A good warm up should last at least twenty minutes, starting at a gentle pace before increasing to full activity.
Some players use compression shorts which can help maintain the temperature of the muscle tissue. Leg supports can also help to retain muscle temperature and some are specifically designed to support the quadriceps muscles.
As with the practice of warming up, players must also be encouraged to have a cool down period; this can help with the transportation of waste materials from muscles and it helps to prevent injury or re-injury.
Return to sporting activity after an injury to the rectus femoris muscle should not be rushed as too early a return often results in re-injury. Finally, a quick accurate diagnosis and appropriate treatment is the key to full recovery.
Footballing Groin Injuries
Groin pain and groin injuries are a frequent hazard associated with playing football. A groin strain is technically an injury to the lower abdominal muscles, but it is also often taken to include an injury to the muscles of the inner thigh. These latter muscles, called the adductors, consist of six muscles that span the distance from the inner pelvis to the inner thigh bone (femur). These muscles pull the legs together, and also help with other movements of the hip joint.
Pain in the groin is a very common occurrence for anyone who plays football. In the early stages, the affected individual may be able to continue playing their sport, but the problem usually gets progressively worse. After sport the sufferer will be stiff and sore. The day after a game, turning or getting out of bed or a car often causes pain, as may coughing, sneezing and sit-ups.
Many people refer to on-going groin (lower abdominal) pain as “sportsman’s hernia” however this is incorrect. The syndrome where chronic groin pain persists, particularly in athletes,was first identified in 1980 by Consultant Surgeon Mr Jerry Gilmore and subsequently labelled “Gilmore’s Groin”. Symptoms include pain during sports movements, particularly hip extension, twisting, turning and kicking. This pain is centred on the lower abdomen but may radiate to the adductor muscle region and even the testicles. The person will usually point to an area of the lower abdomen known as the “superficial inguinal ring” as the main site of the pain, although it can be difficult for the patient to pin-point the exact location.
As pain in the groin and pelvis can result from a number of problems, including injuries to the lumbar spine, the hip joint, the sacro-iliac joint, the abdomen, and the genito-urinary system, diagnosis of “Gilmore’s Groin” requires skillful assessment of the sufferer and is based on the medical history, clinical signs, and, increasingly, an MRI scan.
“Gilmore's Groin” is a complex condition, and many cases are misdiagnosed as a groin strain or a hernia. The injury occurs at the junction of the leg and the torso. It involves the area where the abdominal muscles converge to form the inguinal ligament.
The external oblique muscle has an archway through which several nerves and vessels pass. In “Gilmore's Groin”, a groin muscle tear causes this archway to open up much wider. Further tears in the oblique muscle cause it to lift up and away from the inguinal ligament, leaving the transverse abdominis muscle unsupported. In addition up to 40% of patients diagnosed with “Gilmore’s Groin” may also have torn adductors. Minor and moderate tears usually respond to adductor exercises and physiotherapy. Patients with severe adductor tears usually require adductor tenotomy or release.
The success of surgery for this type of groin injury depends on accurate diagnosis, meticulous repair of each element of the disruption and intensive rehabilitation according to an individualised rehabilitation programme. Surgery is recommended for footballers who are unable to play or fail to respond to rehabilitation. The surgical treatment consists of restoring normal anatomy with a six-layered structural repair of the inguinal region. So, if you are a player suffering with this type of injury it is best to get to a specialist Groin Unit where the repair can be done ideally in the off season when there will be plenty of time to recover from the surgery.
Gilmore Groin Technique
Interestingly, at The Gilmore Groin and Hernia Clinic, following discussion with surgeons from around the world, the classical Gilmore technique has recently been modified with the aim of reducing the recovery time, whilst maintaining the strengths of the full anatomical repair. The formal repair is now known as the Marsh Modification of the Gilmore Technique. 
Many patients also show signs of pubic bone stress injury and in these cases surgery to divide the inguinal ligament as it inserts into the pubic tubercle will reduce the tension (an inguinal ligament tenolysis). In addition, the permanent suture used for the darn has been changed from a large nylon stitch to a smaller, less reactive prolene stitch. Whilst still giving the immediate strength that is required to allow rapid rehabilitation, this stitch should produce less tissue reaction and so less discomfort.
Whilst the risk of injuries then can sometimes be reduced, more often than not they are simply the result of bad luck. Whatever the circumstances, appropriate assessment and treatment is required to ensure that the healing process can take place as quickly as possible.











